Immune Compatibility Test
Immune Compatibility Test
KIR-HLA-C: Immune Compatibility and Maternal-Fetal Tolerance Test
Embryo implantation is the most important step for pregnancy to occur, where the embryo, in the blastocyst stage, attaches to the receptive endometrium. When the uterus is prepared, a short period called the implantation window occurs, during which the embryo implants.
The human immune system is responsible for protecting against pathogens, and for a successful pregnancy, there must be maternal tolerance towards the embryo.
The structures that identify our cells are called HLA (Human Leukocyte Antigen) and consist of two parts (C), one of which we inherit from our mother and the other from our father. On the other hand, Natural Killer (NK) T lymphocytes are the cells responsible for allowing gestation, which bind to the embryo's HLA through KIR (Killer Immunoglobulin-like Receptors).
The KIR-HLA-C genotype is an immunological recognition code that can affect pregnancy and its progression, allowing the risk of embryo rejection by the maternal immune system to be established. It is performed based on the couple's DNA, through a blood sample.
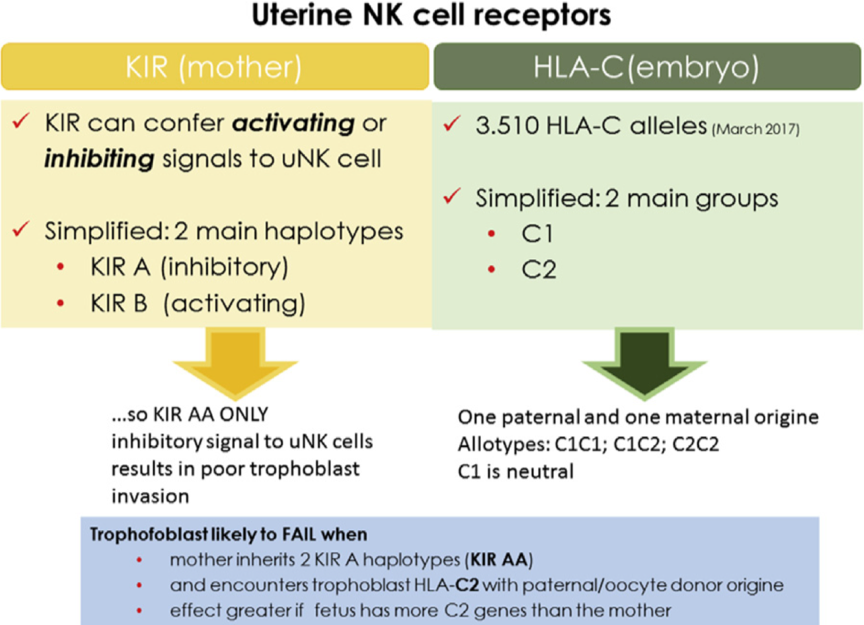
KIR-HLA-C System. Image by Alecsandru. KIR and HLA. Fertil Steril 2017.
Recent studies show that different KIR-HLA-C combinations in the mother and embryo may be associated with an increased risk of infertility, pre-eclampsia, implantation failure, and recurrent miscarriages. This occurs when there is an incompatibility between the embryonic KIR receptors and the identification fragments found on the embryo's surface (HLA-C), one inherited from the father and the other from the mother.
HLA ligands for KIR are divided into two groups: HLA-C (C1) and HLA-C (C2). So far, studies have shown that donor or patient sperm with a C1/C1 combination is more reliable than sperm with a C2/C2 combination. Thus, women with the KIR AA genotype are at increased risk when associated with a paternally inherited C2 gene.
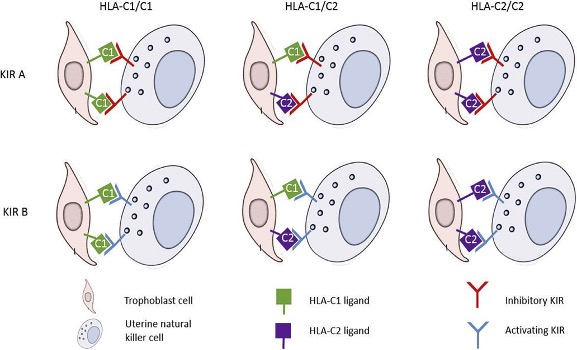
Possible combinations of trophoblastic HLA-C ligands and maternal natural killer cell immunoglobulin receptors (KIR). There are six possible HLA-KIR combinations at the maternal-fetal interface, based on trophoblastic HLA zygosity and maternal KIR haplotype. Image and text modified from Morin. KIR haplotype, HLA ligands, and risk of loss. Fertil Steril 2016.
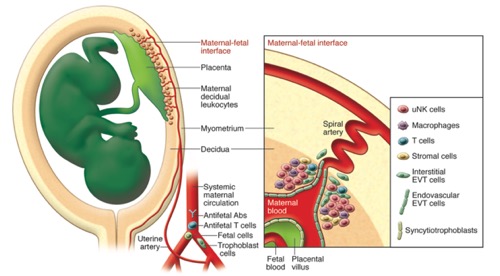
Maternal immune response to the fetus and placenta. The uterine mucosa is in direct contact with the fetal placenta at the maternal-fetal interface. This is the main site where fetal placental cells are in direct contact with maternal tissues. Anti-fetal antibodies and T cells circulate in maternal blood along with fetal and trophoblastic cells. Image and text modified from Moffett A, Colucci F. J Clin Inves. 2014.
Benefits of KIR-HLA-C Genotyping:
- Improve success rates.
- Avoid complications during pregnancy.
- Identify the cause of implantation failures and/or recurrent miscarriages.
- Transfer an appropriate number of embryos.
- Prevent pre-eclampsia.
- Increase accuracy in selecting a donor compatible with the future pregnant woman (both in egg and sperm donation).
In summary, the KIR-HLA-C genotype is a useful tool to improve success rates and reduce the risk of miscarriage in different assisted reproduction treatments. Additionally, it reduces the repetition of treatments and increases the accuracy of donor selection.
Bibliography:
Alecsandru D y col. Hum Reprod. 2014 Dec; 29(12): 2637-43.
Alecsandru D, García-Velasco JA. Fertil Steril. 2017 Jun; 107(6): 1273-1278.
Hiby SE, Apps R, Chazara O, Farrell LE, Magnus P, Trogstad L, et al. Maternal KIR in combination with paternal HLA-C2 regulate human birth weight. J Im- munol 2014;192:5069–73.
King A, Birkby C, Loke YW. Early human decidual cells exhibit NK activity against the K562 cell line but not against first trimester trophoblast. Cell Immunol 1989;118:337–44.
Moffett A, Colucci F. J Clin Inves. 2014; 124 (5): 1872-1879.
Moffett A, Hiby SE. Placenta. 2007; 28 (Supp A): S51-6
Morin SJ y col. Fertil Steril. 2017 Mar; 107(3): 677-683.e2.